
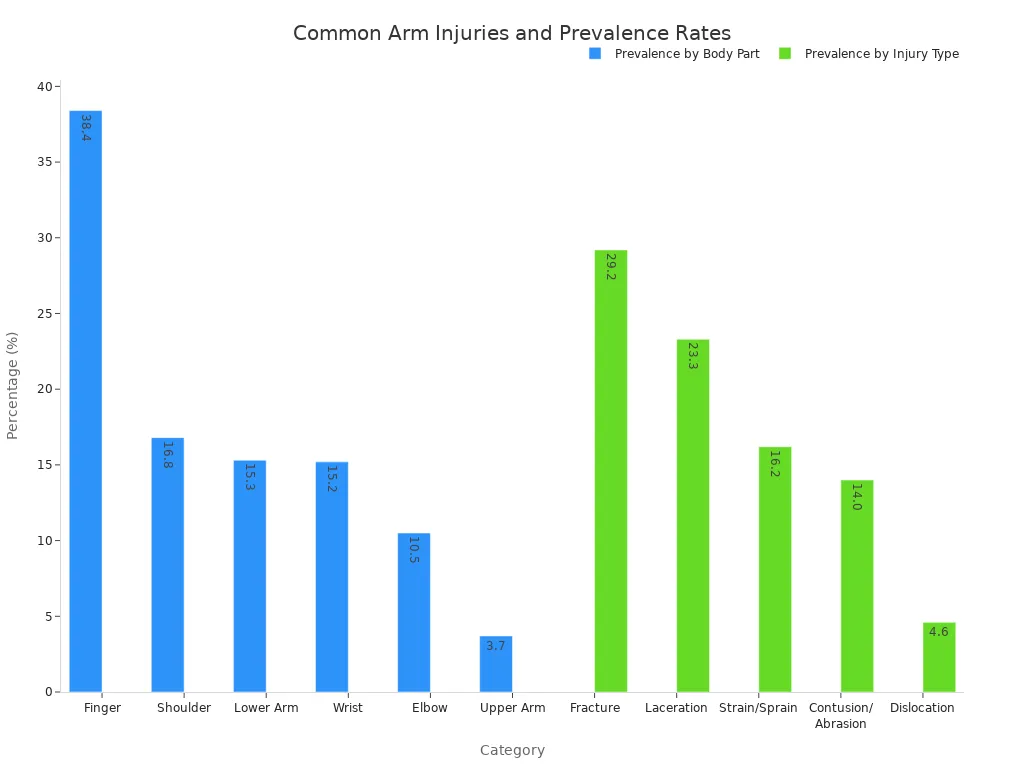
The human arm performs countless daily tasks. Its remarkable capabilities stem from intricate anatomy. Understanding its bones, muscles, and nerves is vital. The arm, despite its strength, faces various injuries. For instance, lower arm injuries account for 15.3% of total injuries. Fractures are also common.
This knowledge helps us appreciate the arm’s function and address problems. This exploration will diagram these essential components of arm anatomy.
Key Takeaways
The arm has bones, muscles, and nerves. They all work together for movement and feeling.
Bones give the arm its shape. Muscles help the arm move and lift things. Nerves send messages to and from the brain.
Keeping your arm healthy is important. Stretching helps muscles and joints. It also prevents injuries.
If your arm gets hurt, rehabilitation helps it heal. This process helps you get back to normal activities.
Understanding your arm’s parts helps you take care of it. This knowledge helps you stay healthy and fit.
Arm Bones: The Skeletal Framework
The human arm relies on a strong skeletal framework. These bones provide structure, protect vital organs, and allow for a wide range of movements. Understanding each bone helps explain the arm’s capabilities.
Shoulder Girdle: Scapula and Clavicle
The shoulder girdle connects the arm to the body’s trunk. It consists of two bones: the scapula and the clavicle. The scapula, or shoulder blade, is a triangular flat bone. It sits on the back of the thorax, usually over the 2nd to 7th ribs.
Its posterior surface has a prominent ridge called the spine of the scapula. This spine extends into the acromion, which forms the point of the shoulder. The scapula also features a shallow glenoid cavity.
This cavity articulates with the humerus. The clavicle, or collarbone, is an S-shaped long bone. It connects the sternum to the scapula. It has a sternal end and an acromial end. The clavicle provides attachment points for several muscles, including the deltoid and pectoralis major.
Upper Arm Bone: Humerus
The humerus is the single bone of the upper arm. It extends from the shoulder to the elbow. This long bone plays a vital role in arm mobility and support. The humerus enables a wide range of arm movements.
These include rotation at the shoulder joint, raising the arm away from the body (abduction), and lowering it toward the body (adduction). It also allows for arm extension and flexion. The humerus serves as a crucial attachment point for many muscles in the shoulder and arm, such as the biceps and triceps.
Forearm Bones: Radius and Ulna
The forearm contains two bones: the radius and the ulna. The radius runs from the elbow to the wrist. It is critical for arm motion and stability. The radius rotates around the ulna, allowing the palm to turn upward (supination) and downward (pronation).
This rotation provides nearly 180 degrees of movement. The ulna is the other forearm bone. Both the radius and ulna transmit loading forces to the elbow and wrist. The radius carries most of the load through the wrist. These bones also provide stability through their joint contours, ligaments, and surrounding muscles.
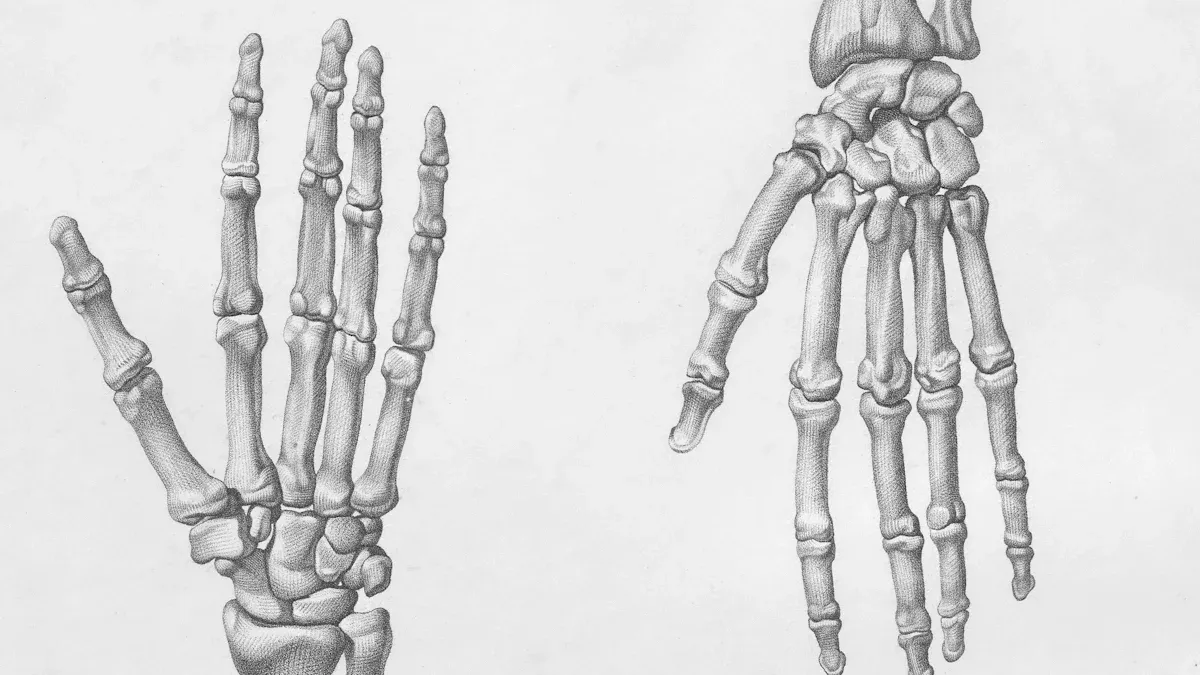
Hand and Wrist Bones
The hand and wrist contain many small bones. The wrist has eight carpal bones. These bones arrange into two rows: proximal and distal. The proximal row includes the scaphoid, lunate, triquetrum, and pisiform. The distal row consists of the trapezium, trapezoid, capitate, and hamate. These carpal bones work together to provide flexibility and strength to the wrist. Beyond the carpals, the hand has metacarpals and phalanges, forming the palm and fingers.
Arm Muscles: Power and Movement
The arm’s ability to perform complex actions comes from its many muscles. These muscles work together, providing power and allowing a wide range of motion. The humerus, the single bone of the upper arm, connects to 13 muscles. These muscles of the arm divide into different compartments. This division helps organize their functions.
Muscles of the Upper Arm
The muscles of the upper arm divide into two main groups: the anterior compartment and the posterior compartment. Each compartment contains specific muscles responsible for different actions.
The anterior compartment of the upper arm houses three key muscles: the biceps brachii muscle, the coracobrachialis muscle, and the brachialis muscle. These muscles primarily contribute to the flexion of the arm at the elbow and shoulder.
The biceps brachii muscle is a prominent muscle. It has two heads, a short head and a long head. These heads have distinct attachments.
Aspect | Description |
|---|---|
Origin | Short head: Apex of the coracoid process of the scapula. Long head: Supraglenoid tubercle of the scapula. |
Insertion | Radial tuberosity of the radius; Deep fascia of forearm (via bicipital aponeurosis). |
Function | Flexion and supination of the forearm at the elbow joint; Weak flexor of the arm at the glenohumeral joint. |
The coracobrachialis muscle also resides in the anterior compartment. This muscle helps move the upper arm.
Origin: Coracoid process of the scapula.
Insertion: Medial side of the humeral shaft, at the level of the deltoid tubercle.
Action: Flexion of the arm at the shoulder, and weak adduction.
The brachialis muscle is another important flexor. It lies deeper than the biceps brachii.
Origin: Medial and lateral surfaces of the humeral shaft.
Insertion: Ulnar tuberosity, just distal to the elbow joint.
Action: Flexion at the elbow.
The posterior compartment of the upper arm contains one major muscle: the triceps brachii muscle. This muscle is crucial for the extension of the arm. The triceps brachii muscle has three heads. Each head has unique attachments.
Aspect | Description |
|---|---|
Origin | Long head: Infraglenoid tubercle of scapula |
Insertion | Olecranon process of ulna |
Actions | Extends forearm; long head extends, adducts arm, extends shoulder |
The triceps brachii muscle’s attachments are detailed below.
Attachments (Origins):
Long head: Infraglenoid tubercle of the scapula.
Lateral head: Humerus (superior to the radial groove).
Medial head: Humerus (inferior to the radial groove).
Attachments (Insertion):
Distally, the heads converge into one tendon. This tendon inserts onto the olecranon of the ulna.
Function (Actions):
Extension of the arm at the elbow.
Forearm Muscles: Flexors and Extensors
The forearm contains many muscles that control wrist and finger movements. These muscles divide into flexors and extensors.
The flexor muscles of the forearm are generally located on the anterior side. They bend the wrist and fingers.
Muscle Name | Primary Functions |
|---|---|
Pronator teres | Pronates and flexes the forearm |
Flexor carpi radialis | Flexes and abducts the hand at the wrist |
Palmaris longus | Flexes the hand at the wrist and tightens the palmar aponeurosis |
Flexor carpi ulnaris | Flexes and adducts the hand at the wrist |
Flexor digitorum superficialis | Flexes the middle and proximal phalanges of the medial four digits, and flexes the hand at the wrist |
The extensor muscles of the forearm are generally located on the posterior side. They straighten the wrist and fingers.
Muscle Name | Primary Functions |
|---|---|
Brachioradialis | Flexes the forearm at the elbow joint. It is most effective when the forearm is in a mid-pronated or mid-supinated position. It also assists in pronation and supination to the mid-position. |
Extensor Carpi Radialis Longus (ECRL) | Extends and abducts the hand at the wrist joint. It works synergistically with the extensor carpi ulnaris for extension and with the flexor carpi radialis for abduction. |
Extensor Carpi Radialis Brevis (ECRB) | Extends and abducts the hand at the wrist joint. It is a stronger extensor of the wrist than the ECRL. |
Extensor Digitorum | Extends the medial four fingers (index, middle, ring, and little fingers) at the metacarpophalangeal (MCP) and interphalangeal (IP) joints. It also assists in extending the wrist. |
Extensor Digiti Minimi | Extends the little finger at the MCP and IP joints. It also assists in extending the wrist. |
Extensor Carpi Ulnaris (ECU) | Extends and adducts the hand at the wrist joint. It works synergistically with the extensor carpi radialis muscles for extension and with the flexor carpi ulnaris for adduction. |
Anconeus | Assists the triceps brachii in extending the forearm at the elbow joint. It also stabilizes the elbow joint during pronation and supination. |
Supinator | Supinates the forearm at the radioulnar joints. It is active during slow, unresisted supination. |
Abductor Pollicis Longus (APL) | Abducts the thumb at the carpometacarpal (CMC) joint and extends the thumb at the CMC and metacarpophalangeal (MCP) joints. It also assists in radial deviation of the wrist. |
Extensor Pollicis Brevis (EPB) | Extends the thumb at the MCP joint and assists in extending the thumb at the CMC joint. |
Extensor Pollicis Longus (EPL) | Extends the thumb at the interphalangeal (IP), MCP, and CMC joints. It also assists in radial deviation of the wrist. |
Extensor Indicis | Extends the index finger at the MCP and IP joints. It also assists in extending the wrist. |
Rotator Cuff Muscles: Shoulder Stability
The shoulder joint is highly mobile. This mobility requires strong support from the rotator cuff muscles. These four muscles of the shoulder form a “cuff” around the head of the humerus. They anchor it within the shoulder socket. They are crucial for maintaining the shoulder joint’s stability and function. They keep the humeral head centered in the glenoid fossa, prevent dislocation, control joint motion for smooth movement, and provide strength during overhead activities.
The four essential rotator cuff muscles are:
Supraspinatus: This muscle controls internal rotation and lifting of the arm. It initiates and acts throughout the range of abduction. It possesses equal abduction power as the deltoid.
Infraspinatus: This muscle enables external rotation of the arm within the shoulder socket. It primarily acts as an external rotator of the shoulder with the arm in a neutral position.
Teres Minor: This muscle assists with arm rotation. It helps with external rotation, particularly when the arm is in 90 degrees of abduction.
Subscapularis: This muscle directs arm abduction. It is the main and strongest internal rotator of the shoulder, providing 53% of total cuff strength. It also acts as a passive restraint in a neutral position.
Coordinated Muscle Action
Complex movements like throwing and lifting involve the coordinated effort of several muscles of the arm and muscles of the shoulder. The rotator cuff muscles provide stability to the shoulder joint. They enable a wide range of rotational movements. The deltoid muscle, with its anterior, middle, and posterior fibers, is crucial for lifting and reaching actions. The trapezius muscle supports the arm by moving the shoulder blade (scapula). These muscles work in harmony. The rotator cuff muscles stabilize, the deltoid moves, and the trapezius adjusts the shoulder blade’s position. This creates a full range of motion. This range of motion is essential for both simple and complex tasks involving the upper arm.
Arm Nerves: Sensation and Control
The intricate network of nerves in the arm provides sensation and controls movement. These nerves act as communication lines. They transmit signals between the brain, spinal cord, and the arm’s muscles and skin. Understanding these pathways helps explain how the arm functions.
The Brachial Plexus: Origin and Branches
The brachial plexus is a complex network of nerves. It originates from spinal nerves C5 through T1. This network forms in the neck and extends into the axilla, or armpit. It gives rise to most of the nerves that supply the arm, forearm, and hand.
Each trunk of the brachial plexus divides into an anterior and a posterior division. This creates six divisions in total. These six divisions then reform to create three cords: the posterior, lateral, and medial cords. These cords receive their names from their position relative to the axillary artery.
The posterior cord forms from the three posterior divisions of the trunks (C5–C8, T1).
The lateral cord forms from the anterior divisions of the upper and middle trunks (C5–C7).
The medial cord is a continuation of the anterior division of the lower trunk (C8, T1).
These cords then branch into the major terminal nerves of the arm. These include the radial nerve, axillary nerve, median nerve, ulnar nerve, and musculocutaneous nerve.
Key Arm Nerves: Median, Ulnar, Radial
Several key nerves emerge from the brachial plexus. They provide specific motor and sensory innervation to different parts of the arm.
The musculocutaneous nerve is a mixed nerve. It originates from the lateral cord of the brachial plexus, typically from spinal nerves C5 to C7. This nerve exits the brachial plexus sheath high in the axilla. It then enters the coracobrachialis muscle. The musculocutaneous nerve primarily innervates the flexor compartment of the upper arm. This includes the biceps brachii and brachialis muscles. It also provides sensory innervation to the lateral aspect of the forearm.
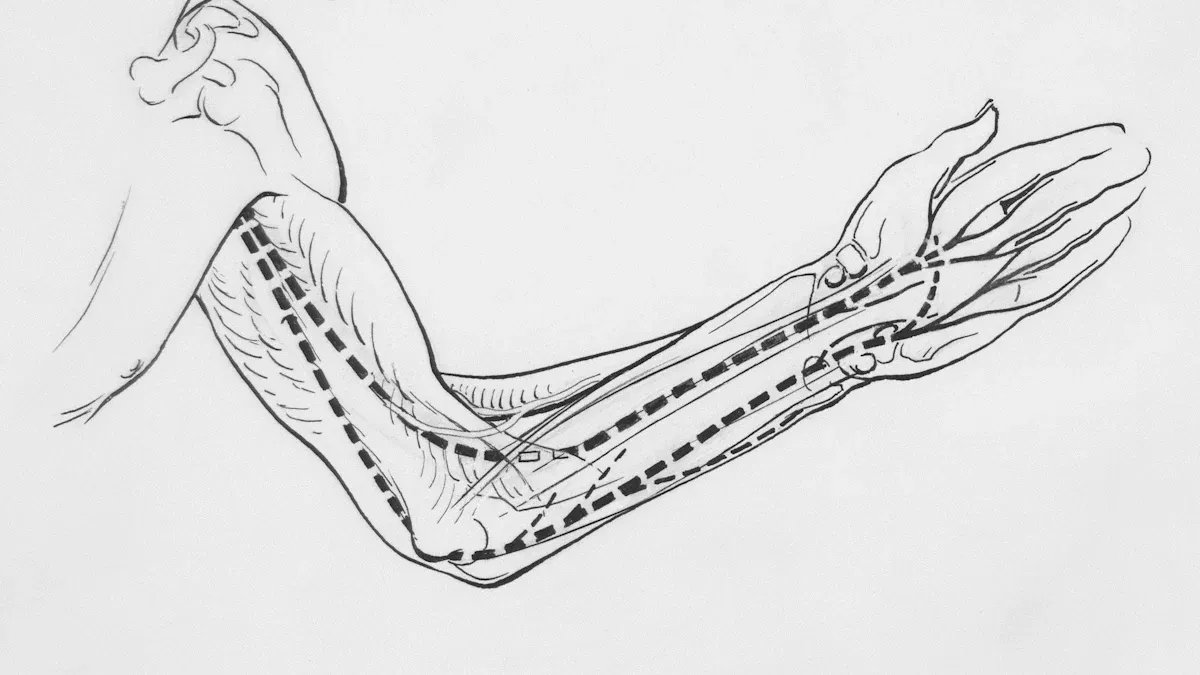
The median nerve travels down the arm and forearm. It provides extensive motor and sensory innervation.
Motor Functions: It innervates the flexor and pronator muscles in the anterior compartment of the forearm. This excludes the flexor carpi ulnaris and part of the flexor digitorum profundus. It also supplies innervation to the thenar muscles and lateral two lumbricals in the hand.
Sensory Functions: It gives rise to the palmar cutaneous branch. This branch innervates the lateral aspect of the palm. It also gives rise to the digital cutaneous branch. This branch innervates the lateral three and a half fingers on the anterior (palmar) surface of the hand.
The ulnar nerve originates from the medial cord of the brachial plexus, specifically from spinal roots C8 and T1. It extends distally through the axilla, arm, and forearm, reaching into the hand.
Motor Functions: Its motor innervation primarily targets the intrinsic muscles of the hand. It also innervates the flexor carpi ulnaris and the medial half of the flexor digitorum profundus in the forearm.
Sensory Functions: Its sensory innervation covers the medial 1.5 digits. This includes the little finger and half of the ring finger. It also supplies sensation to the medial half of the palm and the dorsal surface of the medial one and a half fingers.
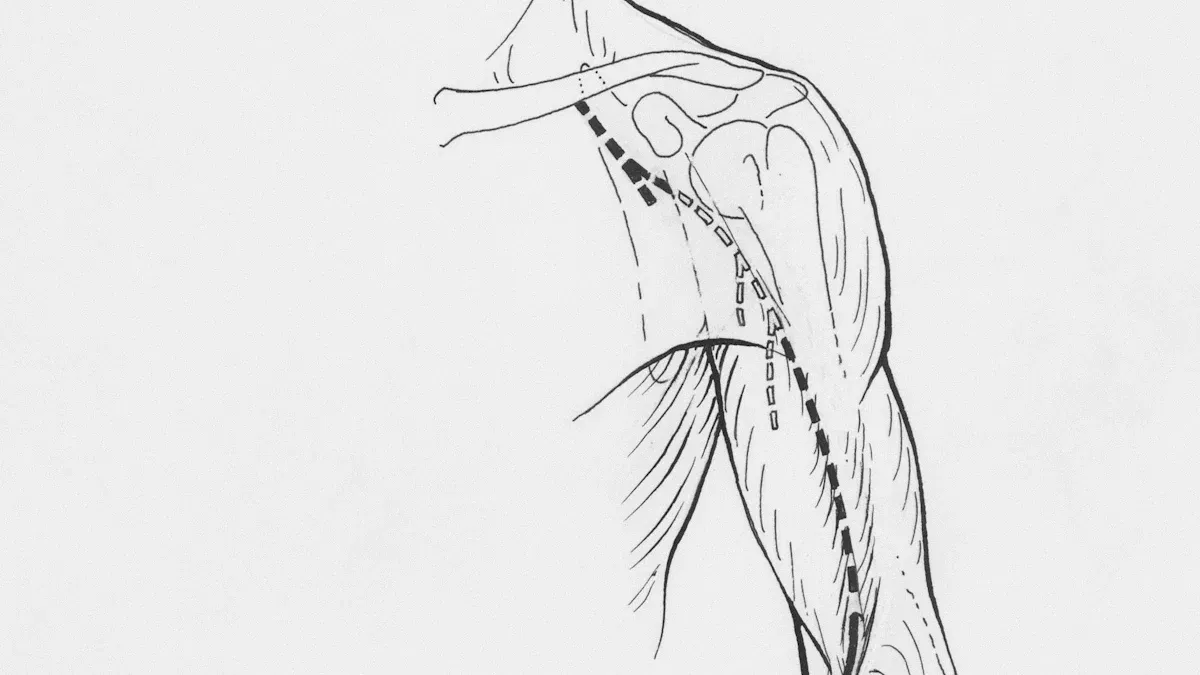
The radial nerve is the largest nerve of the brachial plexus. It wraps around the posterior humerus. This nerve provides motor innervation to the triceps brachii and anconeus muscles in the upper arm. In the forearm, it innervates the brachioradialis and extensor carpi radialis longus. Through its deep branch, the posterior interosseous nerve, it supplies other forearm extensors. These include the extensor carpi radialis brevis, supinator, and muscles that extend the fingers and thumb.
Sensory Innervation: It provides sensation to the skin on the posterior surface of the arm and forearm. It also supplies the lower lateral cutaneous nerve of the arm. The superficial branch of the radial nerve provides sensation to the dorsal aspect of the lateral 3.5 digits (thumb, index, middle, and half of the ring finger) and the radial side of the dorsal hand.
Nerve Function: Signal Transmission
Nerves transmit electrical signals. These signals allow the brain to control muscle movement. They also allow the body to perceive sensations like touch, temperature, and pain. Motor nerves carry commands from the brain to muscles. This causes muscle contraction and movement. Sensory nerves carry information from the skin and other tissues back to the brain. This allows for sensation. This constant two-way communication ensures the arm can react and interact with its environment.
Common Nerve Conditions
Nerves are vulnerable to injury or compression. This can lead to various conditions affecting arm function.
Carpal tunnel syndrome occurs when the median nerve experiences compression within the carpal tunnel in the wrist.
Common Causes: Extra pressure on the median nerve from swelling or damage, repetitive strain injuries, arthritis, sprains, wrist fractures, or ganglion cysts.
Common Symptoms: Numbness, pain, or tingling in the wrist, hand, or fingers (especially the thumb, index, and middle fingers). Symptoms often start at night. They can worsen with repetitive motions. People may experience weakness or clumsiness. This makes gripping objects difficult.
Ulnar nerve entrapment happens when the ulnar nerve becomes compressed or irritated. This often occurs at the elbow (cubital tunnel syndrome) or wrist (Guyon’s canal syndrome).
Common Causes: Activities that stretch the ulnar nerve, prolonged elbow bending during sleep, ganglion cysts, accidents, arthritis, or broken bones.
Common Symptoms: Numbness and tingling sensations in the pinky and ring fingers. People may also experience pain in the elbow or wrist. Hand weakness can occur, leading to difficulty gripping or performing fine motor tasks. In some cases, fingers may develop a claw-like appearance.
Radial nerve palsy results from damage or compression of the radial nerve.
Common Causes: Pressure on the radial nerve (e.g., sleeping on an outstretched arm, compression from crutches), humerus bone fractures, or radial tunnel syndrome (compression in the elbow/forearm). Overuse of the arm and repeated grasping movements are also common causes.
Common Symptoms: Radial nerve pain, burning, itching, tingling, or numbness in the arm, wrist, or hand. Weakness or paralysis in the arm, wrist, or hand can occur. People may have difficulty straightening elbows, wrists, hands, or fingers. A characteristic symptom is “wrist drop,” where the wrist hangs limply and cannot be lifted.
Integrated Arm Anatomy: Function in Motion
The arm’s bones, muscles, and nerves work as a team. This complex system allows for a wide range of movements. Understanding this integrated arm anatomy helps appreciate its capabilities.
Coordinated Movement Example
Throwing a ball shows how bones, muscles, and nerves work together. This gross motor skill needs intricate coordination. Nerves function as the brain’s messengers. They tell muscles when and how to move. Bones serve as structural anchors. Muscles attach to these bones. Skeletal muscles provide the strength and power for movements. This combined action allows complex motor skills like throwing. This intricate anatomy makes such actions possible.
Healthy Arm Anatomy: Prevention and Rehab
Maintaining healthy arm anatomy is crucial. Arm mobility means moving your arm freely without pain. This is important for daily tasks and preventing injuries. Improving arm mobility enhances posture. It reduces injury risk. It also boosts efficiency in daily activities.
Stretching acts as a lubricant for muscles and joints. It promotes movement and pliability. Stretching decreases muscle tightness, soreness, and pain. It helps overworked muscles return to normal length. This improves power and strength. Stretching protects against common arm conditions like tennis elbow. It also enhances blood flow. This brings more nutrients to arm muscles and joints. It improves range of motion.
Here are some simple stretches:
Fingers Up And Down The Stretch: Extend one arm forward at shoulder height. Pull fingers up with the other hand. Hold for deep breaths. Then let the wrist go limp, fingers pointing down. Gently pull on the back of the hand. Repeat on the other side.
Wall Slide: Stand with forearms on a wall at shoulder height. Slide forearms up towards the ceiling. Gently push forearms into the wall. Hold at the top. Slide forearms back down.
Rehabilitation plays a fundamental role in managing arm injuries. This includes rotator cuff issues. Conservative treatment can work for tendinopathies or small tears. When surgery is needed, proper rehabilitation is vital. Early motion often improves range of motion. It leads to faster recovery. Rehabilitation programs are always tailored to the individual patient.
Here is a general protocol for rotator cuff rehabilitation:
Weeks | Protocol |
|---|---|
Phase 1 (0–2) | Strict immobilization; distal hand and wrist active motion allowed. |
Phase 2 (2–6) | Continued immobilization; protected passive range of motion (PROM) initiated; elbow’s active range of motion (AROM) allowed; PROM to active-assistive range of motion (AAROM) at 4–6 weeks. |
Phase 3 (6–12) | Progress from AAROM to AROM with controlled supraspinatus activity. |
Phase 4 (12–20) | Strengthening and endurance exercises with moderate supraspinatus activity. |
Phase 5 (20–26) | Advanced strengthening with higher supraspinatus activity. |
This structured approach helps patients regain function. It reduces pain after injury or surgery.
The arm’s intricate design showcases bones, muscles, and nerves working in perfect harmony. This complex arm anatomy allows for incredible versatility. Understanding this anatomy is crucial for maintaining health and fitness. It also fosters a deeper appreciation for the human body. The arm’s remarkable engineering enables our interaction with the world.
FAQ
What is the main function of the triceps brachii muscle?
The triceps brachii muscle primarily extends the forearm at the elbow joint. Its long head of triceps brachii and medial head of triceps brachii also help stabilize the shoulder. This muscle is crucial for pushing movements.
What is the brachial plexus?
The brachial plexus is a nerve network. It originates from spinal nerves C5 through T1. This network supplies nerves to the arm, forearm, and hand. It controls sensation and movement in these areas.
What is the role of the tendon of biceps brachii?
The tendon of biceps brachii connects the biceps brachii muscle to the radius bone. It helps flex the elbow and supinate the forearm. This tendon is vital for arm movement.
Which muscles does the musculocutaneous nerve innervate?
The musculocutaneous nerve innervates the flexor compartment of the upper arm. This includes the biceps brachii and brachialis muscles. The coracobrachialis muscle also receives innervation. It provides sensation to the lateral forearm.
What is the importance of arm anatomy?
Understanding arm anatomy helps appreciate its function and address issues. It provides insight into how bones, muscles, and nerves work together for movement. This knowledge is key for health and rehabilitation.
