
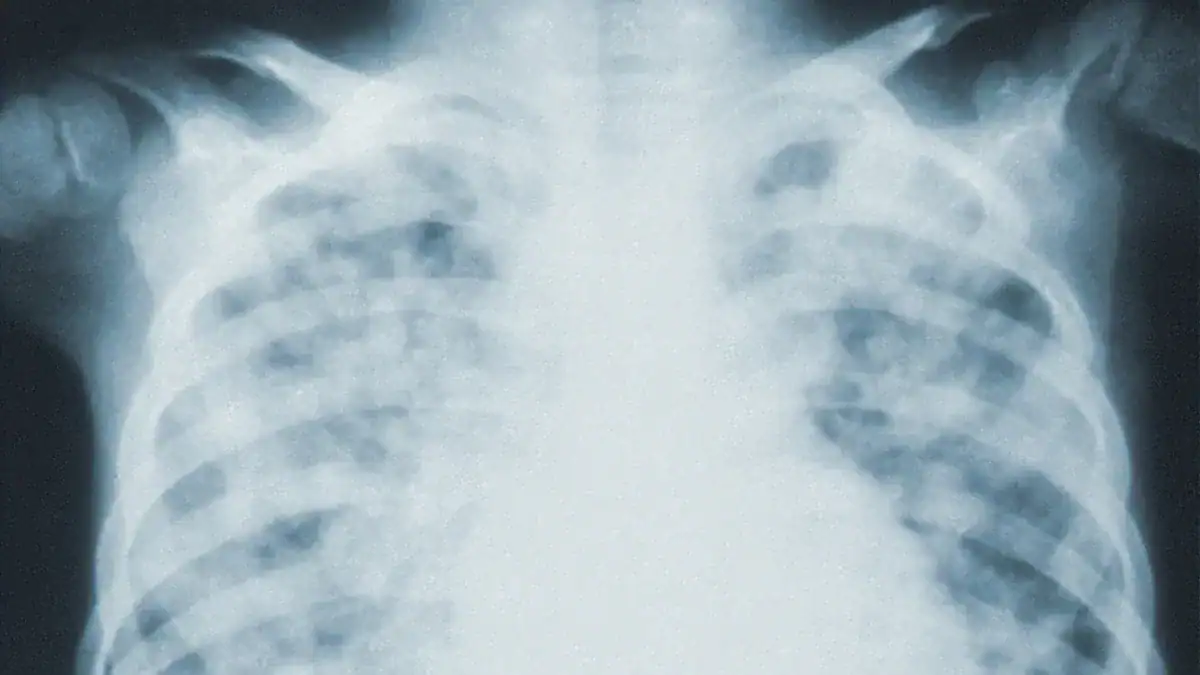
Fluid in lungs, medically termed pulmonary edema, involves an abnormal fluid accumulation within the air sacs of the lungs. This condition severely impedes normal breathing. Pulmonary edema is a serious medical emergency.
It can become life-threatening without immediate treatment. The body does not receive necessary oxygen due to this fluid in lungs. This blog explores the causes, symptoms, dangers, and treatment of this critical pulmonary edema. Understanding this type of edema is vital.
Key Takeaways
- Fluid in the lungs, called pulmonary edema, means fluid fills the air sacs. This makes breathing hard and stops oxygen from getting into the blood.
- Fluid around the lungs, called pleural effusion, means fluid collects outside the lungs. This pushes on the lungs and makes them unable to expand fully.
- Symptoms of fluid in the lungs include sudden shortness of breath, coughing up pink foam, and sweating. Seek medical help right away if you have these signs.
- Heart problems, like heart failure, are a main cause of fluid in the lungs. Other causes include kidney failure, lung injury, and high altitudes.
- Treatments for fluid in the lungs include oxygen, medicines, and fixing the main problem. Managing health conditions and living a healthy lifestyle can help prevent it.
Fluid in the Lungs
Pulmonary Edema Defined
Pulmonary edema describes a condition where excess fluid buildup occurs inside the air sacs of the lungs. These tiny air sacs, called alveoli, normally fill with air. They allow oxygen to enter the blood and carbon dioxide to leave. When fluid fills these air sacs, it makes breathing very difficult. This fluid accumulation prevents the normal exchange of gases. The body does not get enough oxygen. This condition is a type of edema specifically affecting the pulmonary system.
Fluid Around the Lungs: Pleural Effusion
Another condition involves fluid, but it collects in a different place. This is called pleural effusion. It means fluid around the lungs. The lungs sit inside a protective sac called the pleura. This sac has two layers. A small amount of fluid normally exists between these layers. This fluid helps the lungs move smoothly when a person breathes. With pleural effusion, too much fluid collects in this space. This fluid pushes on the lung. It makes the lung unable to expand fully. This differs from pulmonary edema, where fluid is inside the lung tissue itself.
How Fluid Affects Breathing
Both pulmonary edema and pleural effusion make breathing harder. However, they do so in different ways.
With pulmonary edema, fluid fills the air sacs. This fluid makes it harder for oxygen to pass into the blood. It also makes it harder for carbon dioxide to leave. This leads to inefficient blood oxygenation. The body experiences hypoxia, meaning low oxygen levels. The fluid increases the distance oxygen and carbon dioxide must travel. This slows down their movement between the air sacs and the blood. This reduced gas exchange is a major problem.
💡 Tip: Fluid accumulation in the lung air sacs (pulmonary edema) leads to inefficient blood oxygenation, resulting in hypoxia. An increased volume of alveolar fluid heightens the diffusion distance for oxygen (O2) and carbon dioxide (CO2), thereby reducing their rates of diffusion.
Pleural effusion affects breathing by compressing the lung. The fluid outside the lung pushes on it. This limits how much the lung can expand. This compression can make a person feel short of breath. However, the impact on gas exchange can vary. For example, in patients with acute lung injury, pleural effusion often causes greater chest wall expansion. It does not significantly reduce the lung size. It also does not always affect gas exchange or overall respiratory mechanics.
Here is a comparison of how these two conditions impair breathing:
| Characteristic | Pleural Effusion | Pulmonary Edema |
|---|---|---|
| Impaired Function | Compression of the lung, limiting lung expansion | Impaired gas exchange, leading to respiratory distress |
Recognizing Symptoms

Recognizing the symptoms of fluid in the lungs is crucial. Early detection can lead to better outcomes. Both acute and chronic forms of pulmonary edema present different signs.
Acute Symptoms
Acute pulmonary edema develops suddenly. It is a serious condition. People often experience sudden shortness of breath or difficulty breathing. This happens especially when lying down or during activity. Other signs include bubbling sounds, wheezing, or gasping during breathing. A person might cough up pink, frothy sputum. Excessive sweating often accompanies the shortness of breath. The skin can turn blue or gray. Confusion is also possible. A significant drop in blood pressure can cause dizziness or weakness. Some people feel a sense of suffocation or drowning. Cold skin, anxiety, and a rapid, irregular heart rate are also common symptoms.
Chronic Symptoms
Chronic pulmonary edema develops over time. Its symptoms are often less dramatic at first. People might notice a gradual increase in shortness of breath, especially with exertion. Swelling in the legs and ankles can occur. Fatigue and weakness are also common. A persistent cough, sometimes with clear or white sputum, may develop. Waking up at night feeling shortness is another sign. These symptoms of pulmonary edema worsen slowly.
When to Seek Medical Attention
Certain symptoms of pulmonary edema demand immediate medical attention. These signs indicate a medical emergency. Seek help at an emergency room right away. Extreme breathing difficulties or shortness of breath are critical. Feeling like suffocating or drowning requires urgent care. Anxiety related to trouble breathing is a warning sign. A cough producing a pink, frothy mixture of saliva and mucus needs immediate evaluation. Chest pain, a rapid, irregular heart rate, or a blue/gray skin tone are also serious. Sweating accompanied by breathing difficulties means a trip to the emergency room. Do not delay seeking care for these severe symptoms at an emergency room.
Causes of Fluid in Lungs
Many factors can lead to fluid in lungs. Understanding these causes of pulmonary edema helps in proper diagnosis and treatment. These causes fall into two main categories: cardiogenic and non-cardiogenic.
Cardiogenic Factors
Cardiogenic factors relate to problems with the heart. When the heart does not pump blood effectively, fluid can back up into the lungs. This leads to pulmonary edema. Heart conditions are a significant reason for this type of edema. For example, cardiogenic pulmonary edema accounts for 47.8% of cases among patients with Acute Heart Failure.
Heart Failure
Heart failure is a primary cardiogenic cause of pulmonary edema. It means the heart cannot pump enough blood to meet the body’s needs. This inefficiency directly leads to fluid accumulation in the lungs.
Here is how heart failure causes fluid buildup:
- Heart failure impairs the heart’s pumping efficiency.
- Blood backs up into the blood vessels in the lungs.
- Pressure in these blood vessels increases.
- Fluid is pushed from the blood vessels into the air spaces (alveoli) of the lungs.
- This fluid accumulation reduces normal oxygen movement. This leads to shortness of breath.
Congestive heart failure (CHF) represents an imbalance in pump function. The heart cannot adequately circulate blood. This imbalance increases lung fluid. Fluid leaks from pulmonary capillaries into the interstitium and alveoli. Normally, increased lymphatic flow manages fluid transferred to the lung interstitium. This prevents volume increase. However, when lymphatic drainage capacity is exceeded, liquid accumulates in the interstitial spaces around bronchioles and lung vasculature. This causes CHF. Further increases in fluid and pressure can disrupt alveolar membrane junctions. This causes fluid to flood the alveoli and results in pulmonary edema.
Non-Cardiogenic Factors
Non-cardiogenic factors cause pulmonary edema without a direct heart problem. These causes affect the lungs directly or impact the body’s fluid balance. Many different conditions can lead to this type of edema.
Common non-cardiogenic causes of pulmonary edema include:
- Acute Respiratory Distress Syndrome (ARDS)
- High Altitude Pulmonary Edema (HAPE)
- Neurogenic pulmonary edema
- Opioid overdose
- Salicylate toxicity
- Pulmonary embolism
- Reexpansion pulmonary edema
- Reperfusion pulmonary edema
- Transfusion-Related Acute Lung Injury (TRALI)
Other non-cardiogenic causes include:
- Drowning
- Fluid overload
- Aspiration
- Inhalation injury
- Acute kidney disease
- Allergic reaction
Acute Respiratory Distress Syndrome
Acute Respiratory Distress Syndrome (ARDS) is a severe lung condition. It causes fluid to leak into the lungs. This condition often follows a major illness or injury. ARDS leads to widespread inflammation in the lungs. This inflammation damages the tiny blood vessels and air sacs. Fluid then leaks into the air sacs, causing acute pulmonary edema.
Kidney Failure
Kidney failure can also lead to pulmonary edema. The kidneys play a vital role in fluid balance. When kidneys fail, they cannot remove excess fluid and waste products from the body. This leads to fluid overload.
In chronic kidney disease, pulmonary edema typically results from left ventricular failure. This elevates left ventricular filling pressure. It subsequently increases pulmonary hydrostatic pressure.
Other ways kidney failure contributes to edema include:
- Downregulation of epithelial salt-water transporters in the lungs. These transporters are responsible for sodium absorption and passive water follow-up.
- Accumulation of inflammatory cytokines. These include IL-6, IL-8, IL-1β, tumor necrosis factor α, macrophage inflammatory protein 2, nuclear factor-κB, chemokines, and activated innate immune cells. This leads to acute lung injury and ARDS.
The mechanisms include:
- Volume overload (a type of cardiogenic pulmonary edema)
- Left ventricular dysfunction (also a type of cardiogenic pulmonary edema)
- Increased lung capillary permeability (noncardiogenic edema)
- Acute lung injury (noncardiogenic edema with inflammation)
Experimental evidence suggests that noncardiogenic edema and inflammation are present in the lungs following acute kidney injury. This indicates that fluid accumulation alone cannot fully explain the pulmonary edema observed in these patients.
High Altitude Pulmonary Edema
High Altitude Pulmonary Edema (HAPE) is a noncardiogenic form of edema. It commonly affects people who quickly ascend to altitudes greater than 2500-3000 meters. This happens without proper acclimatization.
The primary physiological mechanisms involve exaggerated hypoxic pulmonary vasoconstriction. This elevates pulmonary artery pressure. This can lead to a high-permeability type of edema due to leaks in the capillary wall. This concept is known as ‘stress failure.’ Inhomogeneous pulmonary vasoconstriction can cause regional overperfusion of capillaries. Hypoxic constriction at the level of pulmonary veins can increase resistance downstream of fluid filtration. A diminished capacity for alveolar fluid reabsorption also contributes. Hypoxia inhibits Na+ transporters and decreases transepithelial Na transport. This impairs fluid clearance from the alveoli.
HAPE typically develops in healthy individuals who ascend rapidly to altitudes exceeding 3,000 meters. A critical physiological factor is an excessive increase in pulmonary artery pressure (PAP) before edema forms. This often links to reduced nitric oxide (NO) availability in hypoxic conditions. This leads to an exaggerated hypoxic PAP rise in individuals susceptible to HAPE. The edema itself results from increased microvascular hydrostatic pressure. This leads to the leakage of large proteins and red blood cells across the alveolar-capillary barrier. This phenomenon is sometimes called ‘stress failure.’ Nonuniform hypoxic arteriolar vasoconstriction also plays a role. High blood flow at elevated pressures can exceed the capacity of the alveolar capillary barrier. This disrupts normal fluid balance.
Drug-Induced Edema
Certain medications can cause pulmonary edema. This is known as Drug-Induced Pulmonary Edema (DIPE). The mechanisms vary depending on the drug.
| Medication | Risk Level/Finding |
|---|---|
| Fentanyl | High risk of DIPE |
| Methadone | High risk of DIPE |
| Diazepam | High risk of DIPE |
| Naloxone | Identified with DIPE risk; independent risk factor |
| Dasatinib | Identified with DIPE risk; independent risk factor |
| Nifedipine | Identified with DIPE risk; independent risk factor |
| Anti-thymocyte globulin | Identified with DIPE risk; independent risk factor |
| Pioglitazone | Identified with DIPE risk |
| Cytarabine | Directly damages alveolar-capillary membrane |
| Rosiglitazone | Contributes to fluid retention and increased hydrostatic pressure |
| Verapamil | Induces precapillary vasodilation, leading to fluid redistribution and leakage |
Opioids, such as fentanyl, can induce pulmonary edema. They cause central respiratory depression and trigger sympathetic overactivation. This increases pulmonary vascular permeability. Chemotherapeutic agents like cytarabine directly damage the alveolar-capillary membrane through cytotoxic effects. This compromises its integrity. Thiazolidinediones, including pioglitazone and rosiglitazone, contribute to fluid retention. They elevate hydrostatic pressure within the pulmonary vasculature. Calcium channel blockers, such as verapamil, may induce precapillary vasodilation. This leads to fluid redistribution and subsequent pulmonary leakage.
Other medications that can cause pulmonary edema include:
- Sympathomimetics
- Narcotics
- Salicylates
- Carbamazepine
- Erythromycin
- Hydrochlorothiazide
- IV radiographic contrast agents
- Methotrexate
- Protamine
- Tamoxifen
- Tumor necrosis factor
Other Conditions
Many other conditions can cause pulmonary edema or fluid around the lungs. These include infections, injuries, and certain diseases.
Common non-infectious causes of pulmonary edema include:
- Organ failure: This can involve congestive heart failure, kidney failure, or liver cirrhosis.
- Trauma: Direct injuries to the lungs or other parts of the body can lead to fluid accumulation.
- Reactions to medications: Certain drugs can cause pulmonary edema as a side effect, including overdoses of opioids.
- Brain injuries: Conditions such as brain bleeding, stroke, head injury, brain surgery, tumors, or seizures can lead to fluid in lungs.
- High altitude: Exposure to high altitudes can induce pulmonary edema.
- Blood transfusion: This can sometimes lead to fluid accumulation in the lungs.
- Cardiogenic causes: Problems directly related to the heart, such as fluid overload (from kidney failure or IV therapy), hypertensive emergency, pericardial effusion with tamponade, severe arrhythmias (tachycardia or bradycardia), severe heart failure, or abnormal heart valves.
Infections like pneumonia can cause inflammation and fluid buildup in the lungs. Cancer, especially lung cancer or cancers that spread to the lungs, can also lead to fluid accumulation. Severe injuries, such as chest trauma, can directly damage lung tissue and blood vessels. This allows fluid to leak into the air sacs.
Diagnosing Fluid in Lungs
Diagnosing fluid in the lungs requires a thorough medical evaluation. Doctors use several methods to identify the presence of fluid and determine its cause. This helps them decide on the best treatment.
Physical Exam and History
A doctor begins with a physical exam and reviews a patient’s medical history. They look for specific signs. These include volume gain, reduced tactile vocal fremitus, and dullness on percussion. They also check for diminished or absent breath sounds. Massive pleural effusions can cause respiratory embarrassment and mediastinal shift. The doctor asks about symptoms like dyspnea, a dry cough, and pleuritic chest pain. This pain feels sharp and worsens with deep breaths. A history of pneumonia suggests parapneumonic effusion. Fever indicates an infection. A history of heart, kidney, or liver problems points to transudative edema. Older age, weight loss, and smoking history may suggest malignant pleural effusion.
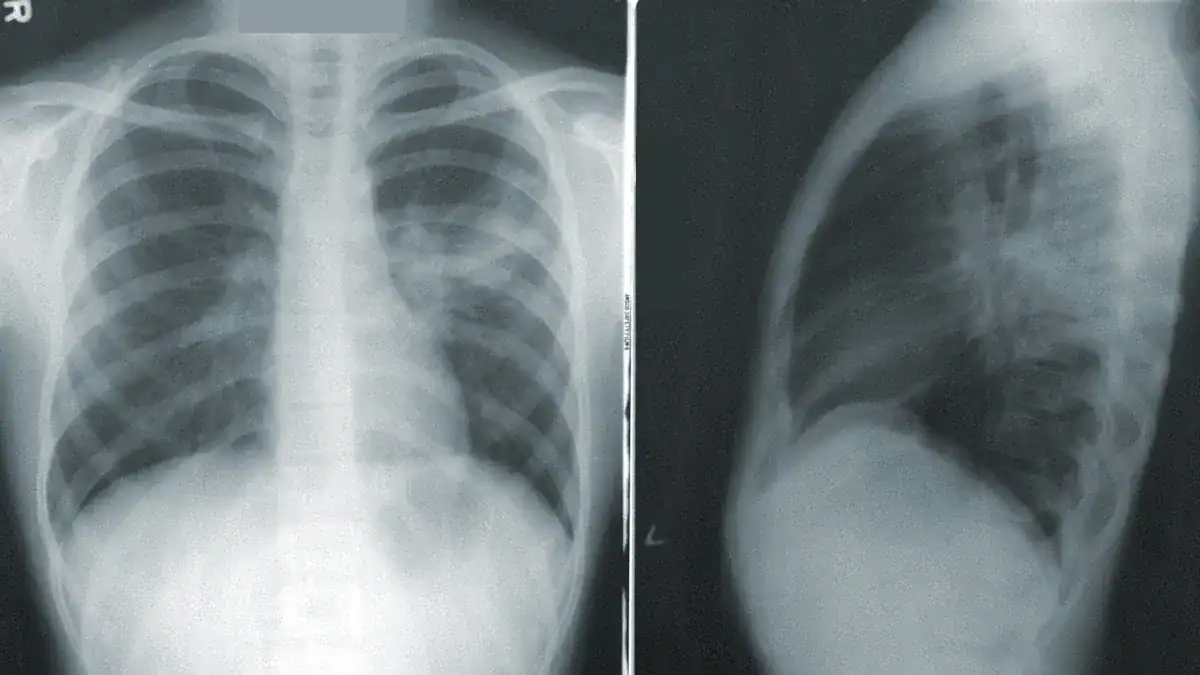
Imaging Tests
Imaging tests are crucial for seeing fluid in the lungs. They help confirm the diagnosis.
| Imaging Test | Sensitivity (%) | Specificity (%) |
|---|---|---|
| Point-of-Care Ultrasound (POCUS) | 83.6–100 | 70–100 |
| Chest X-ray (CXR) | 40–76.2 | 70–97 |
Lung ultrasound (LUS) and chest X-ray (CXR) are common imaging tools. LUS shows higher sensitivity and specificity than CXR for detecting fluid.
Blood Tests
Blood tests provide important clues about the cause of pulmonary edema. Doctors often order a complete blood count and electrolyte panel. Elevated B-type natriuretic peptide (BNP) and NT-proBNP levels strongly suggest heart failure as the cause of the pulmonary edema. Low BNP levels, below 100 pg/ml, indicate a non-cardiac cause is more likely. An arterial blood gas (ABG) test measures oxygen levels. It helps determine the severity of oxygen deprivation. Elevated creatinine levels can point to a cardiogenic cause. An elevated white blood cell count may suggest a non-cardiogenic cause like infection.
ECG and Echo
An electrocardiogram (ECG) and echocardiogram (echo) help differentiate between cardiogenic and non-cardiogenic causes of fluid in lungs. An ECG checks the heart’s electrical activity. An echocardiogram uses sound waves to create images of the heart. It shows how well the heart pumps blood.
| Feature | Cardiogenic Pulmonary Edema (APE) | Non-Cardiogenic (ALI/ARDS) |
|---|---|---|
| Alveolar-Interstitial Syndrome (AIS) | Homogeneous distribution | Dyshomogeneous, with ‘spared areas’ |
| Pleural Line | Regular, normal ‘lung sliding’ | Abnormalities: reduced/absent gliding, thickening, coarse appearance |
| Lung Consolidations | Not characteristic | Typical, especially posterior with air bronchograms |
| Pleural Effusions | More frequent | Less frequent, not reliable for diagnosis |
These tests help doctors understand if a heart problem causes the pulmonary edema. They look for specific patterns. For example, cardiogenic pulmonary edema often shows a homogeneous distribution of alveolar-interstitial syndrome. Non-cardiogenic causes, like ARDS, show dyshomogeneous patterns with ‘spared areas’ in the lungs.
Treatment Approaches
Doctors use various methods to manage fluid in the lungs. The approach depends on the cause and severity of the condition. The goal of treatment is to remove excess fluid and improve breathing.
Emergency Interventions
Acute pulmonary edema requires immediate treatment. Doctors often use nitrates and non-invasive ventilation. These methods have strong evidence supporting their use. Diuretics, such as furosemide, are also given. They help patients with fluid overload. Paramedics successfully resuscitate 60% of patients experiencing cardiac arrest from out-of-hospital pulmonary edema. Prehospital continuous positive airway pressure (CPAP) therapy is feasible for acute respiratory failure. This therapy can prevent the need for endotracheal intubation.
Addressing Underlying Cause
Effective treatment for pulmonary edema focuses on the root cause. For heart failure, diuretic therapy is a primary treatment. It helps manage congestion. Personalized treatment, based on physiological measurements, can improve patient outcomes. For severe heart failure, ultrafiltration or peritoneal dialysis are options. Managing blood pressure and blood glucose is also crucial. Lifestyle changes, like a low-sodium diet and exercise, are important. For kidney failure, dialysis or a kidney transplant may be necessary.
Long-Term Management
Long-term management aims to prevent recurrent fluid in the lungs. For recurrent malignant pleural effusions, doctors recommend indwelling tunneled pleural catheter (ITPC) placement or chemical pleurodesis. For heart failure-associated pleural effusions, thoracocentesis offers symptom relief. Talc pleurodesis is another option for refractory cases. ITPCs are also viable for recurrent benign effusions. This comprehensive treatment helps patients manage their condition over time.
Preventing Fluid in Lungs
People can take several steps to prevent fluid in the lungs. These actions focus on managing underlying health issues and making healthy choices. Preventing pulmonary edema often involves a proactive approach to health.
Manage Chronic Conditions
Effectively managing chronic health conditions significantly reduces the risk of pulmonary edema. These conditions include:
- Heart failure
- Kidney disease
- Lung problems
- High blood pressure
- Diabetes
Individuals with heart failure should follow their cardiologist’s recommendations. They must report any new or worsening symptoms. Maintaining blood pressure within a healthy range helps prevent pulmonary issues. This involves medication, diet, and regular check-ups. Kidney disease or diabetes also require consistent medical oversight. These conditions contribute to fluid retention and can lead to edema.
Lifestyle Changes
Certain lifestyle changes have been scientifically proven to prevent the development or recurrence of fluid in the lungs.
- Limiting salt and fluid intake helps prevent fluid retention and congestion. Sodium causes the body to retain fluid. Avoiding processed foods, canned soups, and salty snacks is crucial.
- Maintaining a healthy weight reduces strain on the heart and lungs.
- Getting early treatment for infections like colds, flu, or pneumonia can prevent worsening heart and lung conditions.
- Eating smaller, more frequent meals can help reduce pressure on the lungs.
- Consuming potassium-rich foods, such as bananas and spinach, supports fluid balance.
Avoid High-Risk Environments
Individuals prone to pulmonary edema should avoid specific high-risk environments or activities. These include:
- Immersion underwater
- Swimming
- Extreme exercise
- Exposure to altitude
Water immersion to any depth can increase risk. Physical exercise augments the cardiovascular effects of immersion. Ambient cold also increases these effects. Compression of the thorax by a wetsuit and negative pressure breathing are additional factors. Avoiding high altitudes, unless medically cleared, is important. Lower oxygen levels at high elevations increase the risk of high-altitude pulmonary edema (HAPE) for individuals with heart or lung conditions. These precautions help prevent pulmonary edema.
Regular Check-ups
Regular medical check-ups are essential. They help monitor chronic conditions and detect early signs of fluid buildup. Doctors can adjust treatments as needed. This proactive monitoring helps manage overall health and prevent complications like edema.
This blog explained pulmonary edema, or fluid in lungs, and fluid around the lungs. It detailed their diverse causes and critical symptoms. Recognizing these signs is vital. Untreated pulmonary edema poses severe dangers. It can lead to life-threatening complications. Individuals must manage underlying conditions and adopt healthy lifestyles for prevention. Understanding the causes helps. Seek immediate medical attention for symptoms of pulmonary edema. Consult healthcare professionals for personalized advice and treatment of this pulmonary edema.
FAQ
What is pulmonary edema?
Pulmonary edema means fluid collects inside the air sacs of the lungs. This fluid makes breathing difficult. It prevents oxygen from entering the blood properly. This condition is a serious medical emergency.
How does pleural effusion differ from pulmonary edema?
Pleural effusion involves fluid gathering around the lungs, in the space between the lung and chest wall. Pulmonary edema, however, means fluid is inside the lung’s air sacs. Both conditions make breathing harder.
What are the main symptoms of acute fluid in the lungs?
Acute fluid in the lungs often causes sudden shortness of breath. People might cough up pink, frothy sputum. They may also experience sweating, anxiety, and a rapid heart rate. These symptoms require immediate medical attention.
What are the two main categories of fluid in lung causes?
The two main categories are cardiogenic and non-cardiogenic. Cardiogenic causes relate to heart problems, like heart failure. Non-cardiogenic causes affect the lungs directly or impact fluid balance, such as kidney failure or ARDS.
