

An osteochondral defect involves damage to both the cartilage and the underlying bone within a joint. This specific type of osteochondral defect can significantly impact a person’s mobility and overall joint health. Understanding its causes and the path to recovery is crucial.
These defects commonly occur in major joints, including the knee, ankle, and elbow. The overall incidence of osteochondral defects in the general population is estimated at 15 to 30 per 100,000 people. The knee joint, in particular, shows a notable incidence. This chart highlights varying rates across different demographics. For example, an osteochondral injury in the ankle can cause considerable discomfort and limit movement.
Key Takeaways
An osteochondral defect damages both joint cartilage and the bone underneath. This can cause pain and limit movement.
Injuries, repeated stress, and certain health problems can cause these defects. Understanding the cause helps with treatment.
Doctors use imaging like MRI to find these defects. Symptoms include joint pain, swelling, and stiffness.
Treatment can be non-surgical, like rest and physical therapy. Surgery may be needed for larger defects.
Recovery involves protecting the joint and doing exercises. This helps restore movement and strength.
What is an Osteochondral Defect
Defining the Condition
An osteochondral defect is a specific type of injury. It affects two important parts of a joint: the articular cartilage and the bone underneath it. The word ‘osteo’ means bone, and ‘chondral’ refers to cartilage. This shows that the defect involves both tissues. This localized area of damage can make a joint hurt and work poorly. When a person has an osteochondral defect, the smooth surface of the cartilage breaks down. The bone beneath it also gets damaged. This dual damage makes the joint less able to handle normal movements and stress. An osteochondral lesion is another term for this type of injury.
Common Joint Locations
Osteochondral defects can happen in any joint in the body. However, they appear more often in certain joints. The knee is the most common joint where doctors find these defects. Many people experience an osteochondral defect in their knee.
The ankle is another frequent location for this type of injury. An osteochondral defect in the ankle can cause significant pain and limit movement. The elbow joint also sees these defects, especially in athletes. Other joints, like the hip or shoulder, can also develop an osteochondral defect, but this is less common. The specific location of the defect often influences the symptoms a person feels and how doctors treat the injury. For example, an osteochondral defect in a weight-bearing joint like the knee or ankle can be particularly challenging.
Osteochondral Defect Causes
Osteochondral defects develop from various factors. These factors often involve mechanical stress or underlying health issues. Understanding these causes helps in both treatment and prevention.
Traumatic Injury
Traumatic injury is a major cause of osteochondral damage. A sudden, forceful impact can damage both the cartilage and the bone. Common scenarios include sports injuries or falls.
For example, most osteochondral lesions of the talus result from trauma. Studies show trauma causes 93–98% of lateral osteochondral talar injuries and 61–70% of medial osteochondral talar injuries. Almost all osteochondral lesions of the talus that occur after an ankle distortion are preceded by trauma.
Several specific traumatic events frequently lead to these defects:
Knee Ligament Injuries: Injuries to knee ligaments, especially the anterior cruciate ligament (ACL), often involve osteochondral fractures. Valgus stress can create shearing forces that damage the femoral condyle.
Patellar Dislocations: When the kneecap dislocates, it can cause osteochondral fractures in a high percentage of patients. Lateral patellar dislocations show a significant incidence of these fractures.
Hip Dislocations: The hip joint is well-protected. However, dislocations can inflict enough damage to cause osteochondral fractures. Many patients with hip dislocations have fragments in the joint or chondral fractures.
Malleolar Ankle Fractures: Fractures around the ankle bone can lead to acute osteochondral fractures. Arthroscopic assessments often reveal cartilage damage in these cases.
Ankle Sprains: Even purely ligamentous ankle injuries can cause osteochondral damage. An inversion force during plantar flexion or dorsiflexion, often with rotation, creates shearing forces that can result in a defect.
Repetitive Stress
Repeated stress on a joint can also lead to an osteochondral defect over time. This type of injury occurs gradually. It happens when the joint experiences microtraumas that accumulate. Athletes often face this risk due to their activities.
Activities that involve repetitive stress include:
High-Impact Sports: Sports like basketball, football, soccer, gymnastics, and throwing sports place significant stress on joints.
Repetitive Movements: Running, jumping, and pivoting motions can wear down cartilage and bone.
Weight-Bearing Activities: Certain types of weight-lifting can also contribute to the development of a defect.
These repeated forces can exceed the joint’s ability to repair itself. This leads to the breakdown of cartilage and underlying bone. Proper training techniques and rest are important for prevention.
Underlying Conditions
Sometimes, an osteochondral defect arises from an underlying disorder of the bone. These conditions affect the health of the bone and cartilage, making them more vulnerable to damage.
Specific medical conditions linked to osteochondral defects include:
Legg-Calvé-Perthes (LCP) disease: This childhood hip disorder disrupts blood supply to the femoral head. This causes avascular necrosis (AVN) and structural changes. These changes lead to chondral and osteochondral lesions.
Avascular Necrosis (AVN): Compromised blood supply causes the death of bone cells. This weakens the bone. It can lead to microfractures that extend to the articular cartilage. This forms chondral and osteochondral lesions.
Osteochondritis Dissecans (OCD): OCD can cause chondral and osteochondral lesions. It involves repetitive trauma or microtrauma. This disrupts blood supply to the subchondral bone and cartilage. This leads to degeneration and possible detachment of bone and cartilage fragments.
Deficient blood supply to the injured region is a theoretical cause for the development of an osteochondral defect, especially in the knee. While the exact origins of these defects are not always clear, this factor contributes alongside direct trauma and repetitive strain.
Symptoms & Diagnosis

Recognizing the signs of an osteochondral defect early helps in getting proper treatment. Doctors use specific methods to diagnose these conditions accurately.
Recognizing Symptoms
An osteochondral defect often causes noticeable symptoms. These symptoms can vary depending on the affected joint and the severity of the defect. People commonly experience:
Joint Pain: This pain is often persistent or intermittent. It worsens with activity or when the person puts weight on the joint.
Swelling: The affected joint may swell, especially after physical activity or increased use.
Stiffness: A feeling of stiffness or reduced range of motion can occur in the joint.
Locking or Catching: The joint might ‘lock’ or ‘catch’ during movement. This suggests a loose fragment of cartilage or bone.
Instability: The joint may feel unstable or ‘give way’ during weight-bearing or certain movements.
Reduced Mobility: People find it difficult to perform daily activities or participate in sports and physical exercise due to the pain.
Diagnostic Methods
Doctors use several imaging techniques to diagnose osteochondral defects. Magnetic Resonance Imaging (MRI) is a very effective tool. It helps diagnose, quantify, and predict the outcome of articular cartilage problems, including osteochondral defects. MRI can often differentiate the cause of the defect. It also helps locate detached loose bodies inside the joint. MRI can identify signs of unstable lesions. These signs include a high-intensity rim signal, cysts under the lesion, high signal intensity through the cartilage, and fluid-filled defects suggesting complete detachment.
Imaging Modality | Grading System | Key Features for Osteochondral Lesions |
|---|---|---|
X-ray | Berndt and Harty | Trabecular compression, partially detached fragment, completely detached but undisplaced, detached and displaced lesion |
CT | Loomer et al. Modification | Compressed, chip avulsed but attached, detached chip but undisplaced, detached and displaced chip, radiolucent/cystic lesion |
MRI | Hepple et al. | Articular cartilage damage only, cartilage injury with underlying fracture and bony edema, detached but undisplaced fragment, detached and displaced fragment, subchondral cyst formation |
Conventional radiography offers an indirect view of cartilage health. It can detect small pieces of subchondral bone. However, it has limits for early cartilage loss and direct cartilage visualization. Diffraction-enhanced X-ray imaging is an experimental technique. It can directly show articular cartilage. Ultrasound is also a valid tool for assessing articular cartilage. It offers high resolution and is affordable. However, it has limitations for deep joints and depends on the operator’s skill.
Identifying an Osteochondral Lesion
Identifying an osteochondral lesion requires a thorough evaluation. Doctors combine a patient’s symptoms with imaging results. For example, an osteochondral lesion in the ankle often presents with specific pain patterns. Imaging helps confirm the presence and extent of the defect. This is especially true for osteochondral lesions of the talus, which commonly affect the ankle joint. The diagnostic process aims to pinpoint the exact location and nature of the osteochondral damage. This helps doctors plan the most effective treatment for the affected joint.
Osteochondral Defect Treatment

Treating an osteochondral defect aims to reduce pain, restore joint function, and prevent further damage. Doctors consider many factors when they decide on the best treatment plan. These factors include the size and location of the defect, the patient’s age, and their activity level. Both non-surgical and surgical options are available.
Non-Surgical Options
Doctors often try non-surgical treatment first, especially for smaller defects or less severe symptoms. These methods focus on managing pain, reducing inflammation, and allowing the joint to heal naturally. Non-surgical treatment can be effective for many patients.
Here are some common non-surgical interventions:
Weight-bearing restrictions: Patients may need to avoid putting weight on the affected joint. This helps reduce stress on the damaged area.
Non-steroidal anti-inflammatory drugs (NSAIDs): These medicines help reduce pain and swelling.
Physiotherapy: Specific exercises strengthen muscles around the joint. They also improve range of motion and stability.
Casts and Braces: These devices immobilize the joint. They provide support and protect the defect from further injury.
Restricted sports activities: Patients must limit activities that put stress on the joint.
Taping: Taping can provide extra support to the joint.
Activity modification: Changing daily activities helps avoid movements that cause pain.
Prolotherapy: This involves injecting a solution into the joint. It aims to stimulate healing.
Platelet-Rich Plasma (PRP): Doctors inject a concentrated solution of the patient’s own platelets. This can promote tissue repair.
Shockwave therapy: This treatment uses sound waves to stimulate healing in the affected area.
The success rates for non-surgical treatment of osteochondral defects vary. A meta-analysis of 14 studies found a 45% success rate for osteochondral lesions of the talus (OLTs). However, other studies show more promising results. For example, Bauer and colleagues reported 80% good to excellent clinical results in a 20-year follow-up of 23 cases. Shearer and his team found 62% good to excellent results in 26 cases.
A recent study by Seo and others, with a 6-year follow-up on 244 OLTs, showed that only 3% of patients needed surgery due to increased symptoms. Nonoperatively treated patients saw a significant reduction in pain scores and improved function. They also showed no progression of ankle osteoarthritis.
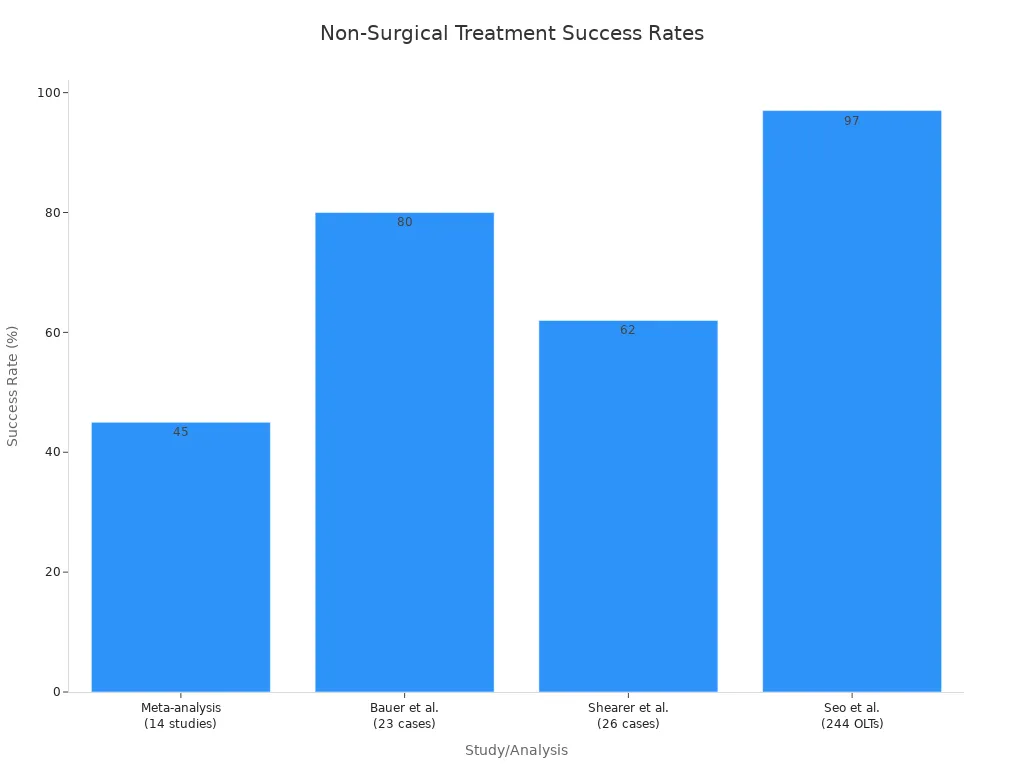
This chart highlights the different success rates observed in various studies for non-surgical treatment.
Surgical Approaches
When non-surgical treatment does not work, or for larger defects, doctors may recommend surgical treatment. Surgical treatment aims to repair or replace the damaged cartilage and bone. The choice of surgery depends on the defect’s size, location, and the patient’s overall health.
Here are some common surgical techniques:
Microfracture: This technique creates small holes in the bone beneath the defect. This allows blood to form a clot. The clot then develops into fibrocartilage to cover the defect. This method works well for small defects in young individuals.
Bone drilling: Doctors drill multiple small holes into the bone. This promotes new blood vessel growth. It enhances healing and new cartilage cell formation.
Osteochondral autograft transplantation: Doctors take healthy cartilage and bone plugs from a non-weight-bearing area of the patient’s own joint. They then transplant these plugs into the defect. This is also known as mosaicplasty.
Osteochondral allograft transplantation: This involves transplanting cartilage and bone plugs from a donor into the defect.
Autologous chondrocyte implantation (ACI) & Matrix-induced ACI (MACI): Doctors harvest healthy cartilage cells from the patient’s knee. They grow these cells in a lab (or on a biodegradable scaffold). Then, they implant them into the defect to promote cartilage repair.
Osteochondral (OCD) repair is a surgical procedure. It fixes a broken piece of cartilage, with or without bone, back to its original location. Doctors use bioabsorbable anchors for this. This technique works for acute injuries. The bone and cartilage fragments must be preserved and large enough for fixation. Alternatively, an osteochondral graft can repair the defect.
Different surgical procedures have varying levels of invasiveness and features:
Surgical procedure | Invasive degree | Features |
|---|---|---|
Mosaic-type osteochondral autologous transplantation (OAT) and microfracture (MF) | HIGH | Patient clinical improvement in OAT and MF; Superior articular cartilage repair in OAT to MF |
MF-combined osteochondral paste | MODERATE | Poor Safranin-O and type II collagen staining in MF group; High GAG content and DNA-normalized GAG; High expression of type II collagen and aggrecan |
MF with hole geometry | HIGH | No significant effect in osteochondral repair |
Recovery & Rehabilitation
Recovery after treatment for an osteochondral defect varies significantly. It depends on the nature of the osteochondral lesion and the specific treatment received. Patients often require a period of immobilization.
Post-Treatment Care
Post-treatment care focuses on protecting the healing joint. For an OATS procedure, strict non-weight-bearing is necessary for the first two weeks. Partial weight-bearing follows between weeks two and four. Full weight-bearing gradually begins from week six to eight.
Microfracture procedures for condylar lesions typically allow touchdown weight-bearing with crutches for six to eight weeks. Nonoperative management for acute, non-displaced osteochondral lesions of the talus usually involves four to six weeks of immobilization. This includes protected weight-bearing. For conservative treatment of ankle osteochondral lesions, immobilization in a cast or walker is common for at least four to six weeks. Patients use crutches and avoid weight-bearing.
Controlling swelling and discomfort is crucial. Early range of motion often begins around week two for many treatments. For marrow stimulation procedures, a fracture boot is used for four weeks. Physical therapy continues, and patients can expect a full return to activity around three months. For particulated juvenile articular cartilage grafts, non-weightbearing lasts four weeks in a fracture boot. Range of motion starts at two weeks, avoiding inversion/eversion. Physical therapy begins at four weeks without axial loading. Non-impact exercises like biking may start at eight weeks.
Rehabilitation Stages
Rehabilitation is a structured process. It aims to restore joint function. A comprehensive rehabilitation program helps patients regain strength and mobility. Regaining range of motion is especially important for knee recovery. Specific exercises help achieve this.
Quadriceps sets improve knee extension. Patients lie on their back, push the knee towards the ground, and hold for 10-20 seconds. Heel slides aid knee flexion.
Patients slide their heel backward, bending the knee, and repeat. Step-ups strengthen leg muscles. Patients step onto a sturdy surface, then slowly lower themselves. These exercises are vital for a successful recovery.
Osteochondral defects damage both cartilage and bone. Early diagnosis and appropriate treatment are crucial for joint health. Recovery is a process that demands patience and adherence to rehabilitation protocols. Personalized care plays a vital role in successful outcomes. Readers should consult a healthcare professional for advice. They can manage the condition and guide prevention strategies.
