Kidney cysts are common fluid-filled sacs that can form in a kidney. Doctors categorize these kidney cysts as either “simple” or “complex.” This difference is crucial for understanding the significance of any complex cyst.
Simple kidney cysts become more common with age; many individuals over 50 develop these benign cysts, with prevalence significantly increasing in later decades. This guide explains these terms, showing how a kidney cyst size chart helps doctors assess characteristics and potential concerns for any kidney cyst, including complex kidney cysts. We provide clear, actionable information for your kidney health.
Key Takeaways
- Kidney cysts are common fluid-filled sacs. Doctors classify them as simple or complex. Simple cysts are usually harmless.
- The Bosniak classification system helps doctors. It sorts kidney cysts by how they look on scans. This helps decide if a cyst needs watching or treatment.
- Complex kidney cysts have features like thick walls. They might need more attention. This is because they have a higher chance of being cancerous.
- Many kidney cysts do not cause problems. But, if you have back pain, fever, or blood in your urine, see a doctor. These can be signs of a problematic cyst.
- Treatment for complex cysts depends on their type. Options include watching the cyst, draining it, or surgery. Your doctor will choose the best plan for you.
Kidney Cysts
What They Are:
Kidney cysts are common fluid-filled sacs that develop on or within a kidney. These sacs contain liquid and typically do not cause problems for the kidney. A simple kidney cyst often has a well-defined outline and homogeneous features. They can appear as single or multiple cysts, affecting one or both kidneys.
Many individuals are unaware they have a kidney cyst because they are usually asymptomatic. These fluid-filled sacs on the kidney surface are contained by a thin wall and often do not impact overall kidney function.
Main Types:
Doctors classify kidney cysts into two main categories: simple and complex. Simple cysts are benign, meaning they are not cancerous. They appear as well-defined, roundish, anechoic structures on imaging, with an imperceptible near wall and a thin echogenic far wall.
Complex kidney cysts, however, show more intricate features. These can include thick walls, internal echoes, septations, or calcifications. Any lesion not meeting the criteria for a simple cyst is considered complex. These features indicate a higher potential for malignancy, making complex cysts a greater concern for the kidney.
How Common Are Kidney Cysts:
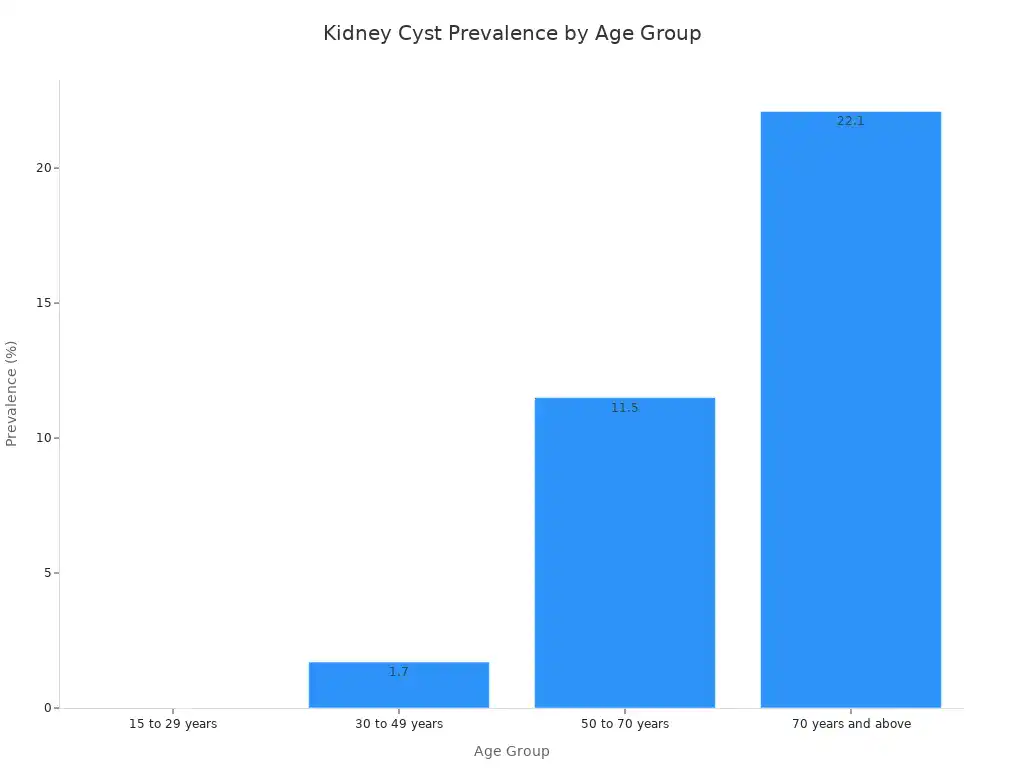
Kidney cysts are very common, and their prevalence increases significantly with age. For example, only 6% of people aged 21 to 40 years have kidney cysts. This number rises sharply for older individuals. Over 35% of people over 70 years old have kidney cysts. The presence of a kidney cyst becomes more likely as a person ages. The chart below illustrates this trend clearly, showing how the percentage of individuals with kidney cysts grows across different age groups.
| Age Group | Prevalence of Kidney Cysts |
|---|---|
| 21 to 40 years | 6% |
| > 70 years | 35% |
The Kidney Cyst Size Chart: Simple vs. Complex
Doctors use a specialized system to classify kidney cysts. This system helps them understand the nature of a cyst and its potential risk. The Bosniak classification system is a primary tool for diagnosing renal cystic masses larger than 1 cm. It helps manage incidental findings of complex renal cysts.
This system has undergone refinements over time, including a 2019 update. It now formally incorporates MRI findings and provides more specific definitions for imaging terms. The Bosniak classification defines five categories of cystic renal lesions. These categories are I, II, II-F, III, and IV. They stratify the risk of malignancy in cystic renal masses.
Bosniak Classification
The Bosniak classification system categorizes kidney cysts based on their appearance on imaging, especially CT scans. This system helps doctors determine the likelihood of a cyst being cancerous. It guides decisions on whether a cyst needs monitoring or treatment. The categories range from simple, benign cysts to those with a high chance of malignancy.
Simple Cysts (Bosniak I)
Bosniak I cysts are the most common type. They are considered benign. These are typically simple kidney cysts. They have thin, smooth walls and contain only fluid. Imaging shows no septa (internal divisions), calcifications, or solid components. Doctors do not consider them cancerous.
The malignancy risk for Bosniak I cysts is very low, reported as 3.2%. This figure comes from pooled estimates across 89 Bosniak I lesions. Simple kidney cysts can vary significantly in size. They range from a few millimeters to several centimeters. For example, they can be from 5mm to 9cm. The average size of Stage I renal cysts is typically 5–10 mm in diameter. However, they can be larger. Most kidney cysts tend to be less than 2 inches wide.
Minimally Complex Cysts (Bosniak II)
Bosniak II cysts show some features that make them slightly more complex than simple cysts. However, they are still almost certainly benign. These cysts might have a few thin septa or fine calcifications in their walls. They do not show any measurable enhancement after contrast injection. Imaging criteria for classifying a cyst as Bosniak II include:
- Homogeneous lesions with Hounsfield Units (HU) of 21-30 on single-phase portal venous studies.
- Masses evaluated with a renal-specific contrast protocol having HU > 20 and showing no enhancement.
- Thin-walled cystic masses with enhancing septa and/or any type of calcification. The septa must be few (1-3) and thin (≤ 2mm).
- Homogeneous masses with HU of -9-20 or ≥70 on non-contrast CT.
- Lesions too small to characterize but otherwise homogeneous and low-attenuating.
- Cystic masses measuring <30 HU in the portal venous phase on contrast-enhanced CT.
- Well-defined homogeneous masses on non-contrast CT measuring between -9 to 20 HU or >70 HU.
- Well-defined homogeneous masses on unenhanced MR that are hyperintense on T1 (around 2.5x normal parenchymal intensity) or have T2 signal intensity similar to CSF.
- Small masses (up to 1.5cm in diameter) that appear homogeneous, even with pseudoenhancement. Doctors consider these benign Bosniak II lesions.
- A small amount of calcium or lining in the wall or septa of a lesion, if all other US and CT criteria for a cyst are present.
- Hyperdense renal cysts (e.g., containing old blood) on non-contrast CT. They appear isodense or hypodense compared to renal parenchyma after IV contrast. This applies if they are smooth, round, sharply marginated, homogeneous, do not enhance with contrast, do not change configuration, and are 3 cm or less in size.
Follow-Up Cysts (Bosniak IIF)
Bosniak IIF cysts are a step up in complexity. They have features that are not quite benign enough for Bosniak II but not suspicious enough for Bosniak III.
These cysts might have more septa, slightly thicker walls, or minimal enhancement. Doctors recommend follow-up imaging for these cysts. This helps ensure they do not change over time. For Bosniak IIF masses, the recommended follow-up protocol involves computed tomography (CT) or magnetic resonance imaging (MRI) every 2 years.
Indeterminate Cysts (Bosniak III)
Bosniak III cysts are indeterminate. They have a significant chance of being malignant. These cysts show thick, irregular walls or septa. They also show measurable enhancement after contrast. The malignancy risk for Bosniak III cysts is generally cited as approximately 40–60%.
However, various studies have reported different rates, ranging from 41% to 84%. One particular study found a malignancy risk of 60% for Bosniak III renal lesions. A retrospective review of Bosniak III renal cystic lesions, classified by CT and MRI, revealed that 15 out of 25 (60%) were malignant. All malignant lesions were low Fuhrman grade (1 or 2) and showed no progression. Smaller lesions (under 4 cm) were more frequently malignant than larger ones. No patients developed metastatic disease during a three-year follow-up.
Malignant Cysts (Bosniak IV)
Bosniak IV cysts are clearly malignant. They have large, enhancing solid components. These cysts require surgical removal. They represent a high risk of cancer. This kidney cyst size chart helps doctors identify these high-risk lesions.
Size and Features
The size of a kidney cyst and its specific features play a crucial role in its classification. The Bosniak classification system is a key part of the kidney cyst size chart concept. It helps doctors assess the risk of malignancy.
| Bosniak Classification | Mean Size (cm) | Malignancy Rate (Surgically Resected) |
|---|---|---|
| III | 4.37 | 79.3% |
| IV | 4.01 | 84.8% |
This table shows that both Bosniak III and IV cysts, which are complex in nature, have similar mean sizes. However, they carry high malignancy rates when surgically resected.
For Bosniak IIF cysts, those smaller than 2.0 cm were observed to be more likely to regress compared to larger cysts. This finding relates to regression and not directly to the likelihood of malignancy. A long-term follow-up study on simple kidney cysts concluded that initial cyst size did not predict the malignancy tendency. The study explicitly states that it is arbitrary to make clinical decisions based on a larger cyst size. Therefore, while size is a factor, the internal features and enhancement patterns are more critical for determining if a kidney cyst is complex and potentially cancerous.
Symptoms and Concerns
Common Symptoms
Many people with kidney cysts experience no symptoms at all. Doctors often discover these cysts during imaging tests for other conditions. However, some individuals do develop symptoms, especially if a cyst grows large or becomes complex. Common symptoms include upper abdominal pain or dull aches in the back or sides of the body.
Large kidney cysts can cause obstructive symptoms if they press on other organs. These symptoms might include dyspepsia, abdominal pain, or distention. Some people report a lack of bowel movement or flatus. If complications like infection or rupture occur, symptoms can intensify. These intensified symptoms might include pain on the side, stomach pain, back pain, fever, more frequent urination, or blood in the urine.
When to Seek Care
Certain symptoms indicate an urgent need for medical evaluation. You should seek care if you experience fever or back pain. These symptoms can suggest an infected kidney cyst.
Blood in the urine is another serious sign, possibly indicating a bleeding cyst. Pain in the side, back, or upper abdomen also warrants attention, especially if cysts enlarge and press on other organs. Other signs of infection, such as chills, also require medical review. Rarely, kidney cysts can block blood or urine flow through the kidney, or impair kidney function. These situations also require prompt medical attention.
Potential Complications
Untreated or growing kidney cysts can lead to several complications. Large kidney cysts can compress surrounding kidney tissue or blood vessels. This compression can contribute to high blood pressure.
Multiple or very large kidney cysts can interfere with normal kidney function. This is particularly true in conditions like polycystic kidney disease. This interference can lead to kidney failure, where the kidney cannot remove waste effectively. Kidney cysts can also occasionally bleed, causing blood in the urine. This bleeding can lead to further complications. In some cases, cysts in the kidney can increase the risk of heart problems or even brain aneurysms.
Diagnosing and Monitoring Cysts
Imaging for Diagnosis
Doctors use imaging tests to find and characterize kidney cysts. Ultrasound is often the first test. It easily recognizes simple, fluid-filled kidney cysts. These cysts appear with clear borders and homogeneous content.
For cysts that are not immediately considered completely benign, a triple-phase CT scan of the kidneys is the investigation of choice. This scan provides information on internal enhancement and wall thickening. Contrast-enhanced CT is the preferred method for evaluating complex kidney cysts.
It uses narrow detector thickness and intravenous contrast. This helps detect thin septa and small enhancing nodules. It also helps differentiate solid components. MRI is another option when CT is not suitable, such as for patients with contrast allergies. MRI can reveal septa less apparent on CT. It can also show definitive enhancement. This helps in the diagnosis of kidney problems.
Lab Tests
Lab tests help doctors understand overall kidney health. They usually involve blood and urine samples. Blood tests check kidney function by measuring creatinine and urea levels. High levels can mean the kidney is not working well. Urine tests can detect blood or protein. These can be signs of kidney issues. These tests do not directly diagnose a cyst. They help assess its impact on the kidney.
Monitoring Cysts
Monitoring kidney cysts depends on their classification. Simple cysts often need no follow-up. Doctors may recommend follow-up imaging for Bosniak IIF lesions. These are more complex than category II lesions.
They have malignancy rates between 5–25%. The recommended duration and frequency of follow-up are not clearly defined. Follow-up can range from 1 to 5 years. The specific interval depends on the complexity of the cyst. For stable small renal masses, follow-up can be discontinued or extended beyond 5 years. However, there is no consensus on when to safely stop follow-up. Regular check-ups ensure the kidney remains healthy.
Treatment for Complex Kidney Cysts
Doctors determine the best treatment for a complex kidney cyst based on its classification, size, and symptoms. The goal is to manage the cyst effectively and ensure kidney health.
Watchful Waiting
Watchful waiting is an option for some complex kidney cysts. This approach involves regular monitoring with imaging tests. Doctors often recommend watchful waiting for cysts that show low risk or are very small. For patients with a Bosniak III or IV complex renal cyst measuring 2 cm or less, active surveillance is sometimes the preferred management strategy. This table outlines typical management based on the Bosniak classification:
| Bosniak Classification | Malignancy Rate | Management |
|---|---|---|
| Bosniak IIF | 5% | Follow-up imaging (CT or MRI) at 6 months, 12 months, then annually for 5 years. |
| Bosniak III | 50% | Surgical excision or ablation (though small ones may be watched). |
| Bosniak IV | 100% | Surgical excision or ablation. |
Aspiration and Sclerotherapy
Aspiration and sclerotherapy is a minimally invasive procedure. A doctor drains the fluid from the cyst using a needle.
Then, they inject a sclerosing agent, like alcohol or polidocanol, into the cyst. This agent helps the cyst walls stick together, preventing it from refilling. This procedure is often effective for symptomatic simple or less complex cysts. Recent studies show radiological success rates from 60% to 98%. Polidocanol often has a higher success rate (90% versus 61%) compared to ethanol. Overall, the success rate for this treatment ranges from 70% to 95%.
Surgical Options
Surgical intervention is necessary for many complex kidney cysts. Doctors recommend surgery for complex renal cysts classified as Bosniak IIF or higher. They also consider surgery for symptomatic cysts or incidental complex ones.
These cysts require further characterization due to the risk of malignancy or other effects on the kidney. Surgical options include laparoscopic cyst decortication, where surgeons remove part of the cyst wall. For cysts with a high risk of cancer, doctors may perform a partial or total nephrectomy. This involves removing part or all of the kidney.
Managing Infected Cysts
An infected kidney cyst requires prompt treatment. Doctors typically prescribe antibiotics to clear the infection. If antibiotics are not enough, they may drain the infected cyst. This helps remove the pus and fluid. In some cases, surgical removal of the infected cyst may be necessary to prevent recurrence and protect the kidney.
Causes and Risk Factors
Simple Cyst Causes
Simple kidney cysts often form when a nephron tube swells and fills with fluid. Researchers suggest an injury or microscopic blockages in the kidney tubules may lead to these simple kidney cysts. Experts believe weakened kidney tissue forms fluid-filled pouches. These pouches expand and create a cyst. Simple kidney cysts are not inherited. Their likelihood increases with age, especially for individuals over 50.
PKD and Genetics
Polycystic Kidney Disease (PKD) is a genetic condition causing many cysts to grow in the kidney. It has two main inheritance patterns. Autosomal Dominant Polycystic Kidney Disease (ADPKD) is the most common.
Individuals inherit one mutated copy of the PKD1 or PKD2 gene from a parent. PKD1 mutations often lead to more severe disease. Autosomal Recessive Polycystic Kidney Disease (ARPKD) occurs when a person inherits two altered copies of the PKHD1 gene, one from each parent. Parents are usually carriers and do not show symptoms.
Acquired Cysts
Acquired kidney cysts develop due to other medical conditions. Chronic kidney disease (CKD) and kidney failure are common causes. These cysts are more common in individuals undergoing kidney dialysis. The likelihood increases with the duration of dialysis. Dialysis treatments themselves do not cause the cysts. They are a consequence of the underlying chronic kidney disease or kidney failure.
Other Risk Factors
Several non-genetic factors can increase the risk of developing kidney cysts. Age is a significant factor; simple kidney cysts typically affect people 50 and over. Chronic kidney disease (CKD) or kidney failure can lead to acquired cystic kidney disease. Dialysis also tends to affect people on treatment for acquired cystic kidney disease.
Other risk factors include gender, with males appearing to develop cysts more often than females. High blood pressure and smoking also increase the risk of a kidney cyst.
Understanding the difference between simple and complex kidney cysts is vital. The kidney cyst size chart, based on the Bosniak classification system, helps assess risk for each kidney cyst.
Most kidney cysts are benign and need no intervention for the kidney. However, complex kidney cysts require closer attention and further evaluation of the kidney. Early detection and proper medical guidance are key to managing kidney cysts effectively. Always communicate openly with your healthcare provider for personalized advice regarding your kidney health and any kidney cyst.